- DE
- EN
Individual assessment of arteriosclerosis by empiric clinical profiling
Mittwoch, 28. November 2007
Marcus Mutschelknauss, Marco Kummer, Jürgen Muser, Steve B. Feinstein, Peter M. Meyer, Barbara C. Biedermann
Individual assessment of arteriosclerosis by empiric clinical profiling
PLoS ONE 2007; 2:e1215
Background: Arteriosclerosis is a common cause of chronic morbidity and mortality. Myocardial infarction, stroke or other cardiovascular events identify vulnerable patients who suffer from symptomatic arteriosclerosis. Biomarkers to identify vulnerable patients before cardiovascular events occur are warranted to improve care for affected individuals. We tested how accurately basic clinical data can describe and assess the activity of arteriosclerosis in the individual patient.
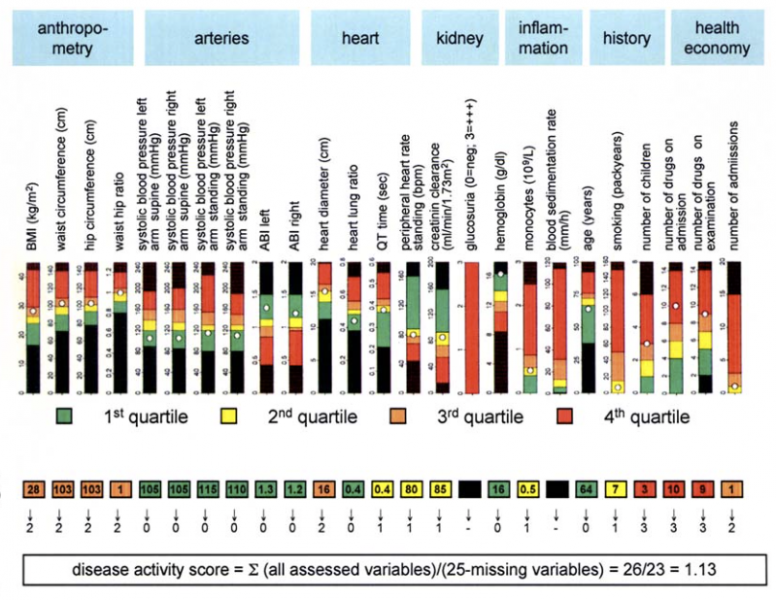
Methodology/Principal Findings: 269 in-patients who were treated for various conditions at the department of general medicine of an academic tertiary care center were included in a cross-sectional study. Personal history and clinical examination were obtained. When paraclinical tests were performed, the results were added to the dataset. The numerical variables in the clinical examination were statistically compared between patients with proven symptomatic arteriosclerosis (n=100) and patients who had never experienced cardiovascular events in the past (n=110). 25 variables were different between these two patient groups and contributed to the disease activity score. The percentile distribution of these variables defined the empiric clinical profile. Anthropometric data, signs of arterial, cardiac and renal disease, systemic inflammation and health economics formed the major categories of the empiric clinical profile that described an individual patient’s disease activity. The area under the curve of the receiver operating curve for symptomatic arteriosclerosis was 0.891 (95% CI 0.799-0.983) for the novel disease activity score compared to 0.684 (95% CI 0.600-0.769) for the 10-year risk calculated according to the Framingham score. In patients suffering from symptomatic arteriosclerosis, the disease activity score deteriorated more rapidly after two years of follow-up (from 1.25 to 1.48, P=0.005) compared to age- and sex-matched individuals free of cardiovascular events (from 1.09 to 1.19, P=0.125).
Conclusions/Significance: Empiric clinical profiling and the disease activity score that are based on accessible, available and affordable clinical data are valid markers for symptomatic arteriosclerosis.
Download: